
Variants v. Vaccines
The Race between the Tortoise and the Hare

German, Italian, Spanish, Hungarian and Japanese translations.
2021 promised to save us. The vaccines were finally here. It was a matter of time. Then B117 arrived, exploded in England, collapsed its healthcare system, and spread across the world.
Each country is now in a race between new variants—the English one, the South African one, and the Brazilian one—and mass vaccinations to stop them. What will happen in your country? Will it be saved by vaccines? Or will it suffer like the UK a new wave of deaths?
When will you get back to the new normal?
To answer that, let’s understand what happened in the UK, gather what we know about B117, look into the vaccines, and forecast what will happen between now and the summer.
What Happened in the UK?

As Alex White has said in the middle of the 3rd wave:

At the peak, one in every 1,000 brits was diagnosed with COVID every day. And it wasn’t due to better testing.

Where did these cases come from?

Nearly all new cases were from England. It’s still crumbling.
This new strain, now called B117, went from nearly non-existent in England to taking over a few weeks. Look at how quickly it happened

Another way to look at the same data:

This growth happened there during a lockdown.

“During the Christmas break, London’s restrictions were equivalent to the national lockdown, with schools closed for the holidays and most offices shut—and still cases grew.”
Cases plummeted only after an even stricter lockdown. This tells us we can beat the new English variant. But to understand exactly how and when we will be able to stop it, we need to understand the variants better.
B117, the English Variant
It Grows 50% to 70% Faster
The best estimates are that it grows between 50% and 70% faster than the previous mainstream variants.
It doesn’t sound much, until you realize that means ~60% more infections this week, and yet again 60% more next week, and again the week after that… Within a couple of months, you have 70 times more cases.
It Can Turn a Dream Story into a Nightmare
If countries had a hard time stopping it before, they will have a much much harder time now. If it’s 60% more infectious, the transmission rate R0 has gone from 2.7 to ~4.3 on average: Lacking any measure and without any immune people, one infected person infects 4.3 others. If a country has few cases because it applied measures that dropped R from 2.7 to, say, 0.9, now those same measures only leave R at ~1.4 (a 60% increase over 0.9). The difference between 0.9 and 1.4 is the same as night and day:

It’s Harder to Stop
Lowering R from 2.7 to 1 is a reduction of 60%.
Lowering R from 4.3 to 1 is a reduction of 75%.
Those 15 additional percentage points might not seem like much, but they are. Countries always start with the most efficient measures: cheap and impactful, such as limiting crowds or mandating masks. As they keep adding measures to reduce R, they become more and more expensive for a smaller impact. So the first 15% in reduction of R is much, much cheaper than going from 60% reduction to 75% reduction.
In many Western countries, that’s when they resort to curfews and closing non-essential businesses (even if there are much cheaper measures).
Herd Immunity Is Farther Away
We just increased the herd immunity threshold from ~60% of the population (through vaccines or recoveries) to ~75-80%.
If in a country 20% of the population is immune after getting infected at some point, with the previous variant it would only have had to vaccinate an additional ~40% of the population to reach the 60% herd immunity threshold.
Now, with a threshold of 75%, instead of an additional 40% of the population to vaccinate, it’s 55%. That’s 35% more vaccines (55% is 35% more than 40%), at a time when vaccines are scarce.

That’s not just harder. It also takes more time. If a country can vaccinate on average 5% of its population per month, it would take 8 months to get to herd immunity with the previous variant (so it would be done by August of 2021). But with the new variant, it would take 3 more months, all the way to November.
And that assumes those who were infected in the past are still immune. As they learned in Manaus, Brazil, this might not be true: They thought they had reached herd immunity with up to 75% of people having been infected1. Then they had a second wave, probably with the new Brazilian variant, they ran out of oxygen, and people died like flies.
It’s Deadlier
When B117 first appeared, most people said: “We shouldn’t worry, normally when viruses mutate they become less virulent.”
I was one of the few who alerted that it was, unfortunately, probably deadlier.

This was the common thinking: "If a virus kills more quickly, it has fewer opportunities to spread. It's the transmission-virulence tradeoff." Unfortunately, that was too simplistic.
The evidence of the transmission-virulence tradeoff theory is not that clear. This fantastic paper explains it well.

The devil is in the details. For example, in the early stages of a pandemic, when most people aren't infected (the case now with COVID), virulence tends to be highest. That includes now, since we’re very far away from herd immunity.

Virulence also tends to increase when the population is highly connected, as we are with COVID, which travels worldwide.

This is what happened in the 1918 pandemic. The first wave, in March-May, was less deadly than the second wave that winter.
When a virus is better at penetrating cells (as this variant is), it means it probably infects many more cells, reproduces faster, and spreads through the body faster, which means it’s harder to stop, which means it kills more. So the more lethal variants are the ones that win. This was known 150 years ago. It’s called passage.
To predict whether this virus was going to be deadlier, we had to turn to specifics.
How COVID behaves made it an unfortunate candidate to increase virulence. Look at this graph of contagions per day after the initial infection. Most infections happen before getting symptoms or early thereafter.

If a variant reproduced more quickly, symptoms would appear earlier and more intensely, which means more transmission early on. The blue and green areas here would have higher peaks.
Also, asymptomatics account for ~50% of infections but don't cause more than 5% of them. A virus that reproduces faster would make many more of them infectious. That means the area that is orange today would become dramatically bigger.
Conversely, because people get sicker and die faster, they will infect fewer people later on, which cuts the right leg of this graph.
The combination of these two factors results in this shift in the curve, from blue to orange:

On balance, which one is bigger? The increase in transmission at the peak would outweigh the reduction in transmission on the right leg.
More sick people would mean more deaths. But deaths happen weeks after infection, so killing people faster won’t reduce the transmission rate. Death and contagiousness are so disconnected with COVID that there's no pressure for the virus to become less deadly.
And this is why the new variant is, indeed, 30% deadlier.

The Race: Variant v. Vaccine
Worldwide Spread
The B117 is in over 80 countries now, and counting. It’s very hard to tell exactly how much of it is in each country, because outside of the UK and Denmark few countries have a proper sequencing system. But this is the closest I could get.

In some countries such as the UK, Israel, Ireland or Austria, B117 is prevalent enough that they’re already feeling its wrath. For the rest of the countries, when will they?

B117 nearly doubles every week. By the end of February, it will account for a majority of cases in Sweden, France, Belgium, Germany, Spain, Netherlands, Italy, Ireland, Luxembourg, Portugal, Switzerland, and Denmark. In those countries, the transmission rate is about to increase by up to 50% through the month. In the US, it will be in mid-March.
So which one will win, the variant or the vaccine? In one country, the winner has already been the vaccine.
Israel
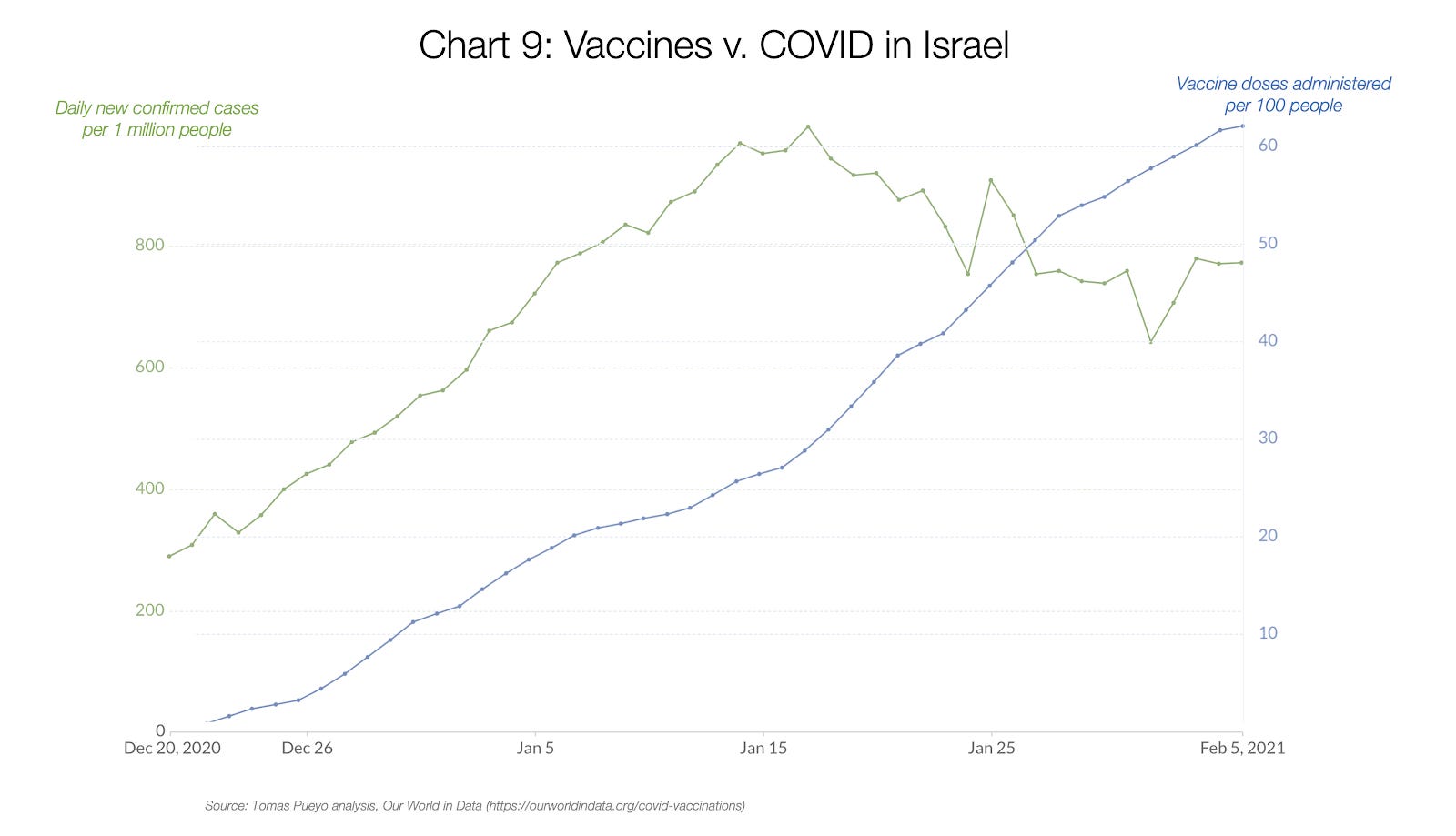
Israel has administered 60 doses of the vaccine for every 100 people. They have seen a reduction in the transmission rate of around 40%. They started feeling the effect in mid-January, when around 30% of the population had received a shot.
Israel could do this as a small developed country with an efficient, centralized healthcare system. Oh, and they paid nearly double per vaccine. Pfizer saw the benefit of more money and a quick real-life test with a country that could deliver, and it became a no-brainer for them to send their vaccines there.
The rest of countries, unfortunately, can’t follow as fast.
Vaccines

The UK and the US aren’t as fast as Israel, but they’re moving forward. At this pace, in 3-4 months the UK might have vaccinated most people. The US will probably take until the summer. In the developed world, the laggards are the Europeans.
To understand why this is happening, we need to understand each vaccine. There are 5 vaccines with Phase III trials available in Western countries. All of them are, in broad terms, very effective.

The 5 vaccines nearly eliminate all severe diseases, even for the new variants. They also eliminate most symptoms for the traditional variant, and in general they eliminate at least 50% of cases for any variant. The only one that is giving more problems right now is the South African variant, but there are still good vaccines against it.
Even if new vaccines didn’t work well with new variants, it would now be pretty easy to adapt. Since we know the genetic code of the variants, small tweaks to the vaccines would likely increase their efficacy while maintaining the same side-effects on humans. My guess is that this isn’t something we should worry about. What we should worry about is that we can’t vaccinate fast enough.
So where’s the problem? Is it that we haven’t bought enough vaccines? No.

Most developed countries have bought many more vaccines than they need. It’s just that the pharmaceutical companies can’t produce them fast enough.
Vaccine production has been another failure story of the pandemic. Moderna’s vaccine was created in January 2020, 2 days after the genetic code of the coronavirus was published. It took a full year for us to test, approve, produce and distribute. We could have done so much better.
For example, we could have had challenge trials: Pay people to get the vaccine and then get infected—instead of waiting for the infection to happen naturally for some. We could have paid whatever it took for people to decide they wanted to do it. If some people want to do it, sacrificing for the others while making money, why prevent them? This would have pulled in the approval of the vaccine by months, saving hundreds of thousands of lives and billions in the economy.
The list of mistakes in vaccine rollout is limitless.
Why expand production capacity *after* approval instead of early on with public funds? Right now a Pfizer plant in Europe has stopped producing vaccines to expand production.
Why publicly pay for the vaccine doses instead of buying their formulas, so we could then get all pharmaceutical companies to produce them?
Why not get competitors to produce winning vaccines immediately after approval?
Why decide who to vaccinate and in what order after vaccines have been approved, and not before, with all the months we had?
The EU Union delayed the approval of its vaccines by at least one month because it was debating with pharmaceutical companies who had the liability if vaccines didn’t turn out to work. Why? The amount of money saved pales in comparison with the wasted economy by postponing vaccinations by one month.
Why not look at results of the trials as they come in, with Bayesian inference, to update the likelihood of success as we go? If we had seen how good results were as they started appearing, we could have started the approval process, the vaccine production, the organization of their rollout…
Because of all these mistakes, now we’re stuck with billions of vaccines bought and only a few million available. It will take until the summer for a sizable share of the population of developed countries to be vaccinated.
The Tortoise and the Hare
In the race between the variants and the vaccines, the variants are the hare and the vaccines are the tortoise.
We all know that, in the end, the vaccines will win. Like the tortoise. By this summer, in developed countries, vaccination rates will likely range between 50% and 80%. Since there will also be some herd immunity, and summer means outdoors in the Northern hemisphere, it’s likely that the pandemic will die down some time during the summer.
The question is: Will they also be rolled out in time to prevent the new variants from taking over? Now we have our answer: Unfortunately, no.

The B117 variant will probably take over between February and March in most developed countries. That’s without taking into account the Brazilian and South African variants.
Emerging countries are in an even worse position: Not only will they have the 3 variants. They will also receive vaccines much later. And in the Southern hemisphere, they’re now enjoying summer. Winter, with more variants and not enough vaccines, might be less forgiving.
So keep tight for a few more months. Don’t let your guard down. The end of the tunnel is near. Get a vaccine if you can. If not, wait till the summer. By September, we’ll likely be back to the new normal in developed countries. And in emerging ones, let’s hope more vaccines and a fast rollout avoids a repeat of 2020.
Stay strong.
Tomas Pueyo
The Manaus data might have been biased, since it wasn’t a random sample. As a result, it’s possible that herd immunity wasn’t achieved, and that the reduction in cases was a combination of natural herd immunity and behavioral changes. It’s also possible that herd immunity was achieved but that the reinfection rate was high with the new variant. More data is needed to know.
Off-topic, but I thought you might find this music geography piece of interest. https://www.honest-broker.com/p/western-music-isnt-what-you-think?isFreemail=true&post_id=144003912&publication_id=296132&r=stzh&triedRedirect=true
Tomas, love the analysis. I would also point out that some vaccines have already been shown to be less effective against variants. So, we may actually end up in a situation similar to influenza (where we have to vaccinate every year). The data out of Manaus, Brazil (that you cited), suggests that.